
Receiving the results of a blood test can often feel like trying to decipher a secret code. You see lists of acronyms, bolded numbers, and reference ranges, but what does it actually mean for your longevity? For decades, the narrative around heart health has been simplified into a battle between “good” and “bad” cholesterol. While this simplification has helped raise awareness, it often misses the nuance required for true preventative health.
Cholesterol is not inherently the enemy; it is a waxy substance essential for building cells, producing hormones, and generating vitamin D. The problem lies not in its existence, but in how it is transported through your bloodstream. For patients navigating heart health, having understanding cholesterol numbers explained in depth is the critical first step toward reducing the risk of cardiovascular disease and stroke.
This guide moves beyond the basics, diving into the lipid panel, advanced metrics, and actionable steps to optimize your metabolic health.
The Lipid Panel: Decoding the Standard Metrics
When your doctor orders a lipid profile, they are looking at how fats (lipids) are circulating in your blood. To get a clear picture of your cardiovascular risk, we must look at the interplay between four distinct values.
1. Total Cholesterol
This is the sum of your blood’s cholesterol content. While it provides a bird’s-eye view, it is often too broad to be a standalone indicator of health. A high total number might not be alarming if your HDL (good cholesterol) is exceptionally high. Conversely, a “normal” total can hide dangerous levels of specific inflammatory lipids.
2. Low-Density Lipoprotein (LDL)
Often branded as the “bad” cholesterol, LDL transports cholesterol from the liver to the arteries. When levels are too high, LDL can deposit on arterial walls, leading to plaque buildup (atherosclerosis). According to the American Heart Association, keeping LDL in check is a primary target for preventing heart attacks.
3. High-Density Lipoprotein (HDL)
HDL is the “garbage truck” of the circulatory system. It scavenges excess cholesterol from the bloodstream and returns it to the liver for excretion. Higher levels of HDL are generally associated with lower heart disease risk, though recent studies suggest that extremely high HDL may not always confer additional benefits.
4. Triglycerides
Triglycerides are the most common type of fat in the body, storing excess energy from your diet. Unlike cholesterol, which builds cells, triglycerides are purely fuel. High levels are often linked to metabolic syndrome, insulin resistance, and uncontrolled diabetes. The Mayo Clinic notes that high triglycerides combined with low HDL or high LDL significantly increases the risk of fatty buildup in artery walls.
Reference Ranges: Where Do You Stand?
Medical guidelines evolve, but the following table represents the general standards set by health organizations for adults. Note that optimal levels can vary based on individual risk factors such as age, smoking status, and family history.
| Metric | Optimal / Desirable | Borderline High | High / Very High |
|---|---|---|---|
| Total Cholesterol | Less than 200 mg/dL | 200–239 mg/dL | 240 mg/dL and above |
| LDL (“Bad”) | Less than 100 mg/dL | 130–159 mg/dL | 160 mg/dL and above |
| HDL (“Good”) | 60 mg/dL and above | 40–59 mg/dL | Less than 40 mg/dL (At Risk) |
| Triglycerides | Less than 150 mg/dL | 150–199 mg/dL | 200 mg/dL and above |
Source: Derived from CDC Cholesterol Guidelines
Beyond Standard Testing: The “Hidden” Risks
If you have a family history of heart disease but your standard panel looks normal, you might need to dig deeper. Modern cardiology is moving toward advanced lipid testing to identify risks that standard tests miss.
Lipoprotein(a) [Lp(a)]
Lipoprotein(a) is a sticky, genetic form of LDL that is highly inflammatory and prone to causing clots. Diet and exercise have little effect on Lp(a) levels because they are determined by your DNA. The National Heart, Lung, and Blood Institute suggests that screening for Lp(a) should be considered for those with premature heart disease in their family tree.
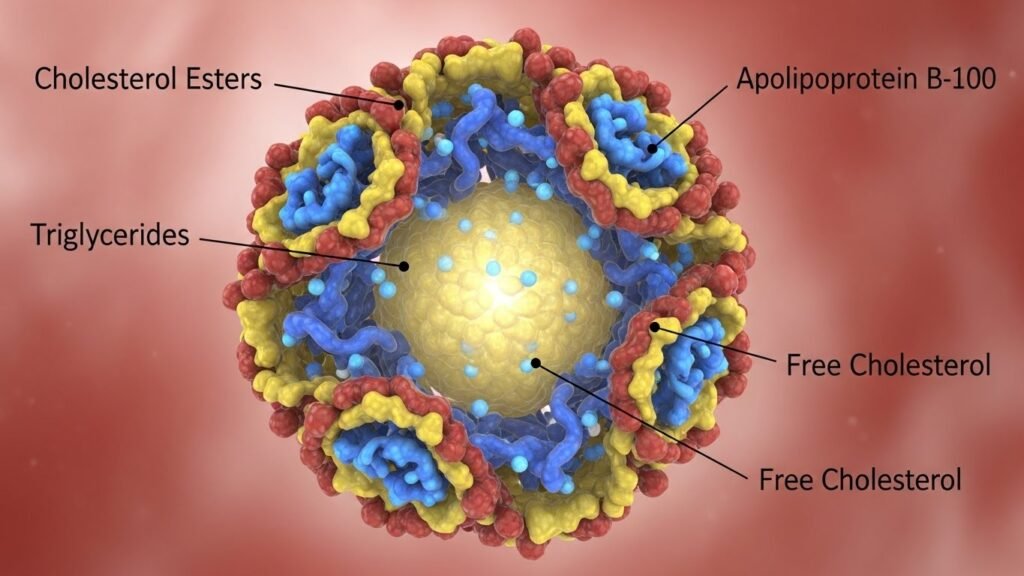
Apolipoprotein B (ApoB)
ApoB is a protein found on the surface of all atherogenic (plaque-causing) particles. Because LDL particles can vary in size—think of them as large beach balls versus small, dense bullets—counting the LDL concentration alone can be misleading. A high number of small, dense particles (high ApoB) is more dangerous than fewer large particles, even if the total LDL mass is the same. Measuring ApoB provides a precise count of the particles capable of clogging arteries.
The Lifestyle Connection: Diet, Movement, and Stress
While genetics play a role (a condition known as Familial Hypercholesterolemia), lifestyle factors are the primary drivers for the majority of the population. Understanding your cholesterol numbers explained in the context of your daily habits empowers you to make changes.
The Fat Debate
Not all fats affect cholesterol equally. Trans fats are universally harmful, raising LDL and lowering HDL. Saturated fats (found in red meat and full-fat dairy) can raise LDL, but the picture is complex. However, replacing saturated fats with unsaturated fats—found in olive oil, avocados, and nuts—is a proven strategy. Harvard Health Publishing emphasizes that a Mediterranean-style diet is one of the most effective ways to manage lipid levels naturally.
The Role of Exercise
Sedentary behavior is a major contributor to low HDL and high triglycerides. Aerobic exercise helps raise HDL and burns triglycerides for fuel. The Cleveland Clinic recommends at least 150 minutes of moderate-intensity exercise per week to see lipid benefits.
The Impact of Sugar
Surprisingly, sugar is often more responsible for poor lipid profiles than dietary cholesterol. Excess sugar intake spikes insulin, which signals the liver to produce more triglycerides and lower HDL. Reducing added sugars and refined carbohydrates is often more effective for improving the lipid panel than cutting out eggs or shrimp.
When Lifestyle Isn’t Enough: Medical Interventions
For some, diet and exercise are not enough to combat high cholesterol, particularly when genetic factors are at play. In these cases, medication becomes a vital tool for longevity.
- Statins: These are the most common cholesterol-lowering drugs. They work by blocking a substance your liver needs to make cholesterol. Information from the FDA confirms their efficacy in reducing cardiovascular events.
- PCSK9 Inhibitors: A newer class of injectable drugs that dramatically lower LDL levels, often used for people who cannot tolerate statins.
- Ezetimibe: This medication prevents the absorption of cholesterol from the intestine.
It is crucial to consult a healthcare provider to weigh the benefits and potential side effects of these treatments. Resources like MedlinePlus offer comprehensive overviews of these medications.
Conclusion: Taking Ownership of Your Heart Health
Cholesterol is not just a set of numbers on a page; it is a dynamic indicator of your metabolic health and future cardiovascular risk. By moving beyond the simple “good vs. bad” narrative and looking at the full picture—including triglycerides, particle size, and inflammation—you can make informed decisions.
Whether through dietary shifts, increased physical activity, or medical intervention, you have the power to influence these metrics. Don’t wait for a cardiac event to take action. Schedule a comprehensive lipid panel with your doctor today, ask about advanced testing like Lp(a), and take control of your heart’s future.
For more global perspectives on cardiovascular health, you can visit the World Health Organization.

